When a patient is switched from a brand-name NTI drug to a generic version, the stakes are higher than with most medications. NTI drugs - narrow therapeutic index drugs - have a razor-thin line between working perfectly and causing harm. Even tiny changes in how much of the drug enters the bloodstream can lead to treatment failure, dangerous side effects, or worse. This isn’t about saving money. It’s about safety. And how you talk to your patient makes all the difference.
What Makes NTI Drugs Different?
Not all drugs are created equal. Most medications have a wide safety margin. If you take a little more or less, your body can handle it. But NTI drugs? Not so much. Take warfarin, for example. Its goal is to keep your INR between 2 and 3. Go below 2? You’re at risk of a clot. Go above 3? You could bleed internally. Now imagine switching from one generic version to another - or from brand to generic - and your INR suddenly shifts. That’s not theoretical. It happens.
Other common NTI drugs include:
- Levothyroxine - even a 5% change in absorption can throw thyroid levels out of balance
- Phenytoin - used for seizures; levels below 10 mcg/mL may trigger seizures, above 20 mcg/mL can cause dizziness or coma
- Digoxin - heart medication; therapeutic range is 0.5 to 0.9 ng/mL. A little too much? Toxic. Too little? Ineffective
- Carbamazepine and valproic acid - both used for epilepsy and mood disorders
The FDA has strict rules for these drugs. While regular generics only need to match the brand within 80-125% of absorption, NTI generics must be much closer: 90-111.11%. For levothyroxine, the standard is even tighter - 95-105% for total exposure. This isn’t just paperwork. It’s science. And it’s why switching isn’t as simple as swapping pills.
Why Do Patients Worry?
Patients aren’t being irrational. They’ve heard stories. A neighbor had a seizure after switching generics. A relative’s INR spiked after a pharmacy change. And yes - research backs up these fears. A 2017 study found that 8-12% of patients with well-controlled epilepsy had breakthrough seizures after switching from brand to generic antiepileptics. That’s not a small number. It’s real.
Even worse, many pharmacists and doctors still hesitate. A national survey showed that while 94% of pharmacists believe generic NTI drugs are safe, only 60% consistently substitute them. Why? Because they’ve seen problems. And they’re scared to make the switch.
Patients pick up on this. If you sound unsure, they’ll be terrified. If you say, “It’s the same thing,” without explaining the science, they won’t believe you. You need to move beyond reassurance. You need to build trust through clarity.
What You Must Say - And How
Don’t just say, “This is fine.” That’s not enough. Here’s what works:
- “This generic version has been tested to deliver the same amount of medicine into your bloodstream as the brand.” Say it like you mean it. Not like you’re reading a script.
- “I prescribe this exact same drug to my own family.” Personal stories build trust faster than data.
- “We’re going to check your blood levels in 7 days to make sure everything is stable.” This isn’t optional. It’s essential.
Use the teach-back method. After explaining, ask: “Can you tell me in your own words why we’re doing this?” If they can’t, you haven’t communicated clearly enough.
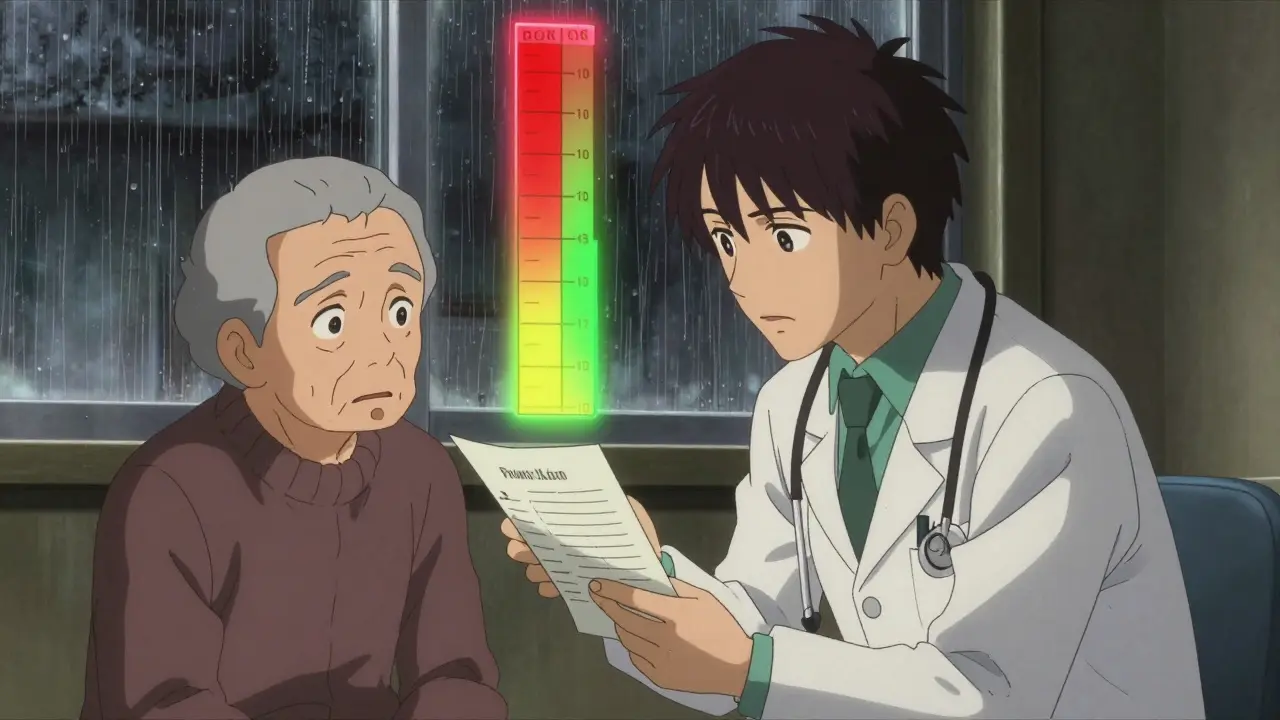
Visual aids help. A simple chart showing the narrow therapeutic window - with a red zone for too low, a green zone for just right, and a yellow zone for too high - makes the risk real. The FDA’s 2024 communication toolkit includes these exact visuals in 12 languages. Use them.
Monitoring Isn’t Optional - It’s the Standard
After switching, you can’t just say, “Call if something feels off.” That’s passive. You need a plan.
- For warfarin: Check INR within 3-5 days. The American Heart Association says this isn’t a suggestion - it’s standard care.
- For levothyroxine: TSH levels should be rechecked in 4-6 weeks. But if the patient is elderly or has heart disease, check sooner.
- For phenytoin or carbamazepine: Serum level checks within 7-10 days. Symptoms like dizziness, nausea, or confusion aren’t normal - they’re warning signs.
Don’t assume the patient knows why they’re being tested. Say: “We’re not doing this because we don’t trust the drug. We’re doing it because we care enough to make sure it’s working perfectly for you.”
State Laws Vary - Know Yours
In 27 U.S. states, pharmacists can’t just switch an NTI drug without your permission. Fourteen of those states require written consent. Thirteen others have specific rules about which NTI drugs can be substituted. If you’re in one of those states, you need to know the law - and make sure your patient does too.
Even if your state allows automatic substitution, you still have a duty to inform. If a patient walks into the pharmacy and gets a different pill without knowing, they might stop taking it. Or worse - they might think it’s not working and double the dose. That’s how emergencies start.
Document everything. Write in the chart: “Patient counseled on therapeutic equivalence of generic [drug] to brand. INR monitoring scheduled for [date]. Educational materials provided.” That’s not bureaucracy. That’s protection.

Who’s at Highest Risk?
Some patients are more vulnerable than others:
- Elderly patients (65+) - slower metabolism, more drug interactions
- Patients with kidney or liver disease - their bodies can’t clear drugs the same way
- Those on 5+ medications - interactions can change how the NTI drug behaves
- Patients with poor adherence - if they miss doses, the risk of instability goes up
If any of these apply, don’t just switch. Have a conversation. Ask: “Have you ever had trouble with this medicine before?” “Do you ever skip doses?” “Do you take other meds from different pharmacies?”
What About Cost?
Yes, generics are cheaper. But that’s not the point here. If you lead with cost, patients will assume you’re cutting corners. Lead with safety. Say: “I know this change might seem small, but with your medication, even a tiny difference can matter. That’s why we’re being extra careful.”
Patients care more about outcomes than price. They want to feel safe. They want to know you’re not rushing them. They want to know you’re watching.
What’s Next?
The FDA is rolling out real-world data tracking in 2025 - using records from 12 million patients to see what actually happens after NTI switches. Early results are promising. For warfarin, generic versions have shown nearly identical absorption - within 97.3% to 101.8% of the brand. That’s tighter than most brand-name versions vary from batch to batch.
But data doesn’t change minds. Communication does. The biggest barrier isn’t science. It’s fear. And fear is only calmed by clear, honest, consistent dialogue.
When you switch a patient to a generic NTI drug, you’re not just changing the pill. You’re changing their trust. Don’t take that lightly. Don’t rush it. And never assume they understand - even if they nod and say yes.
Are generic NTI drugs really as safe as brand-name drugs?
Yes - but only if they meet the FDA’s stricter standards. All generic NTI drugs approved by the FDA have been tested to deliver the same amount of medicine into the bloodstream as the brand. For drugs like warfarin, levothyroxine, and phenytoin, the testing is more rigorous than for regular generics. The 90% confidence interval for absorption must fall between 90% and 111.11%, and for some drugs like levothyroxine, it’s even tighter - 95% to 105%. This isn’t guesswork. It’s science. But approval doesn’t mean zero risk. Monitoring after the switch is still required.
Why do some patients have problems after switching to a generic NTI drug?
Problems don’t happen because the generic is bad. They happen because of changes in absorption, timing, or how the body processes the drug - even if the difference is tiny. Some patients are more sensitive. Elderly patients, those with liver or kidney issues, or people on multiple medications are at higher risk. Also, if the patient switches between different generic brands over time, each switch can cause small fluctuations. That’s why consistent monitoring is critical. It’s not about one switch - it’s about ongoing stability.
Should I always switch a patient to a generic NTI drug?
Not always. If a patient is stable, has had no issues, and is doing well on their current version - especially if they’re elderly or on multiple drugs - there’s no urgent need to switch. The goal isn’t to switch for the sake of cost. The goal is to keep the patient safe and stable. If you do switch, make sure you have a clear plan for monitoring. Never switch without a follow-up test scheduled.
Do I need patient consent before switching an NTI drug?
It depends on your state. In 14 states, written consent is legally required before substituting an NTI drug. In 13 others, substitution is limited or banned for certain drugs. Even if your state doesn’t require consent, it’s still best practice to inform the patient and document the conversation. A simple note like “Patient advised of switch and agreed after discussion” protects you and builds trust.
How long should I monitor a patient after switching to a generic NTI drug?
It varies by drug:
- Warfarin: Check INR within 3-5 days
- Levothyroxine: Check TSH in 4-6 weeks (sooner if elderly or heart disease)
- Phenytoin, carbamazepine: Check serum levels within 7-10 days
- Digoxin: Check levels within 5-7 days
Always schedule the test before the patient leaves. Don’t wait for them to call. Proactive monitoring prevents crises.
George Vou
March 7, 2026 AT 23:15so yeah the fda says its all good but lets be real - i work in a pharmacy and ive seen 3 patients go into seizures after switching generics. they all had the same script. same drug. same dose. but one batch was just... off. like literally. the pill looked different. and the patient swore it didnt feel right. we ignored it. big mistake.
now i check every single ntigeneric like its a bomb. and i tell patients: dont trust the label. trust your body. if you feel weird? call us. dont wait. dont assume. just call.
also... why does the fda even let these things through? theyre not testing real-world absorption. theyre testing in labs with healthy 25-year-olds. what about my 78yo grandma on 7 meds? she dont got time for science.
Ray Foret Jr.
March 9, 2026 AT 15:15hey i just switched my dad to generic levothyroxine last month and everything’s been smooth! 😊 he’s got his tsh checked and it’s perfect. i know people are scared but honestly? the science is solid. my nurse said even the brand-name ones vary by 10% between batches. so why panic? 🙌
just make sure they take it on an empty stomach and dont switch brands mid-stream. consistency > perfection.
Samantha Fierro
March 11, 2026 AT 08:12As a nurse practitioner with over 15 years in cardiology, I want to emphasize that the fear surrounding NTI drug switches is not irrational-it’s informed. Patients are not being difficult; they are protecting their lives.
I always begin with: “I prescribe this to my own mother.” Then I show them the absorption chart. Then I schedule the follow-up bloodwork before they leave the room. No exceptions. No assumptions. And I document every word.
Trust is built not in grand speeches, but in quiet, consistent actions. Never underestimate the power of a scheduled lab order.
Robert Bliss
March 13, 2026 AT 06:36im not a doc but my aunt was on warfarin for 12 years. brand only. then they switched her and her inr went crazy. like overnight. she almost bled out. now she refuses generics. period.
maybe the science says its fine. but i’ve seen what it looks like in real life. and i dont trust it. not even a little.
APRIL HARRINGTON
March 14, 2026 AT 20:31OMG I JUST HAD TO SWITCH MY HUSBAND TO GENERIC PHENYTOIN AND HE STARTED SHAKING AND CRYING AND I THOUGHT HE WAS HAVING A SEIZURE BUT IT WAS JUST TOXICITY???
WE HAD TO GO TO THE ER AND NOW I HATE PHARMACIES AND I HATE THE FDA AND I HATE THAT THEY LET THIS HAPPEN AND WHY IS NO ONE TALKING ABOUT THIS???
THEY NEED TO BAN THIS. LIKE RIGHT NOW. I CANT BELIEVE WE WERE JUST TOLD TO ‘TRUST THE SCIENCE’ LIKE WE’RE A LAB RAT
Leon Hallal
March 16, 2026 AT 10:37you guys are all missing the point. the real problem isn’t the drug. its the system. pharmacies switch brands without telling anyone. no consent. no paperwork. no warning. and then when someone has a stroke or a seizure? oh well. it was just a generic.
the fda doesn’t care. the manufacturers don’t care. and the doctors? they’re too busy to care.
so yeah. the science says its fine. but the system? its a death trap.
Judith Manzano
March 17, 2026 AT 08:23what if the issue isn’t the drug itself, but how often patients are switched between different generic versions? like, if someone gets brand A, then generic X, then generic Y, then generic Z-all within a year-each switch adds a tiny fluctuation. it’s not one switch that’s dangerous. it’s the accumulation.
we need to fix the system, not just the messaging. once a patient is on a generic, lock them in. don’t let pharmacies swap it out unless the prescriber says so.
rafeq khlo
March 19, 2026 AT 05:06the entire narrative is a corporate psyop. the fda’s 90-111% range is mathematically absurd. it allows for a 21.11% variance in bioavailability. that is not therapeutic equivalence. that is gambling with human lives.
furthermore, the studies cited are funded by generic manufacturers. the 2024 data? cherry-picked. the real-world data from 12 million patients? not yet published. because it would prove the opposite.
this is not science. this is capitalism in a lab coat.
Morgan Dodgen
March 20, 2026 AT 22:10let’s be honest-the only reason this is even a debate is because big pharma’s profit margins are collapsing. generics are a threat. so they created this whole ‘narrow therapeutic index’ panic narrative to scare prescribers into keeping the brand-name drugs.
the truth? the brand-name versions are the ones with the real variability. they’re made in 12 different factories across 5 countries. the generic? one clean facility. one batch. one standard.
the FDA’s data is solid. the fear? manufactured.
and yes, i’ve reviewed the raw bioequivalence studies. the variance is negligible. stop being hysterical.
Philip Mattawashish
March 21, 2026 AT 14:31you all are so naive. you think this is about safety? no. this is about control. who gets to decide what you take? the doctor? the pharmacist? or the insurance company? you’re being groomed to accept being a passive patient. to trust the system. to nod and say yes.
the moment you stop asking questions is the moment you lose your body.
if you’re switching a patient to a generic? you’re not helping them. you’re outsourcing their health to a corporation that doesn’t give a damn.
Tom Sanders
March 23, 2026 AT 11:18can we just not? i get it. it’s important. but i’m tired of being lectured about bioavailability and absorption curves. i just want to know: should i switch my mom or not? just tell me yes or no.
Jazminn Jones
March 25, 2026 AT 10:26The assertion that ‘the science is settled’ is not only misleading-it is intellectually dishonest. The bioequivalence standards for NTI drugs are statistically underpowered. The 90-111.11% interval is derived from a sample size of fewer than 24 subjects in most studies. This is not a robust clinical standard. It is a regulatory loophole dressed as science.
Furthermore, the FDA’s own guidance documents acknowledge that inter-subject variability in absorption can exceed 30% in vulnerable populations. Yet we proceed as if this is irrelevant.
This is not safety. This is negligence masked as efficiency.
Stephen Rudd
March 26, 2026 AT 07:00you americans are so dramatic. in australia we switch ntigenerics every day. no one dies. no one has seizures. we have universal healthcare and no one is getting ripped off. why is this a crisis here? because you’re all obsessed with lawsuits and fear. the drug works. get over it.
also your doctors are lazy. if they spent 5 minutes explaining instead of 20 minutes documenting, patients wouldn’t be terrified.
Erica Santos
March 26, 2026 AT 19:17oh wow. so the real villain here isn’t the generic drug-it’s the patient’s ability to tolerate uncertainty. we’ve turned medicine into a religion where ‘trust the process’ is the only prayer that matters.
we don’t need more data. we need more humility. if you’re afraid to switch a patient because you don’t know how their body will react… then maybe you shouldn’t be prescribing.
the fear isn’t in the pill. it’s in the doctor’s hesitation.
Scott Easterling
March 27, 2026 AT 10:22so... if i switch a patient to generic warfarin, and then their inr goes from 2.4 to 3.8 in 48 hours... who’s responsible? the pharmacist? the doctor? the manufacturer? the patient? the fda? the insurance company? because someone’s gonna get sued. and i dont wanna be that guy.
so i just leave them on the brand. even though it costs 10x more. because i’d rather lose money than lose a patient.
and honestly? i’m proud of that.
Samantha Fierro
March 28, 2026 AT 15:31Thank you for sharing your experience. Your point about responsibility is critical. That’s why I’ve started using a standardized consent form: ‘I understand this switch may require closer monitoring. I agree to follow up with bloodwork within 5 days.’ I get their signature. I scan it. I file it. And I say: ‘This isn’t about liability. It’s about care.’
Patients respond to that. They feel seen. Not scanned.