
Ever felt that searing burn in your chest after a spicy dinner or a late-night snack? You aren't alone. For millions of people, that "heartburn" isn't just a one-off occurrence; it's a chronic struggle. When these symptoms happen regularly, it's often GERD is Gastroesophageal Reflux Disease, a chronic condition where stomach acid leaks backward into the esophagus, irritating the lining of the food pipe. While it might seem like a minor nuisance, leaving it unchecked can lead to serious complications. The goal isn't just to stop the burning, but to heal the esophagus and prevent long-term damage.
Why Your Stomach Acid Is Moving Upward
To understand how to fix the problem, you have to understand the "valve." At the bottom of your esophagus sits the Lower Esophageal Sphincter (LES), a ring of muscle that acts as a one-way door. It opens to let food into your stomach and then clamps shut to keep acid where it belongs. In people with GERD, this valve doesn't close properly. Because the esophagus doesn't have the same thick, protective mucus layer that the stomach has, the acid (which typically has a pH between 1.5 and 3.5) literally burns the tissue.
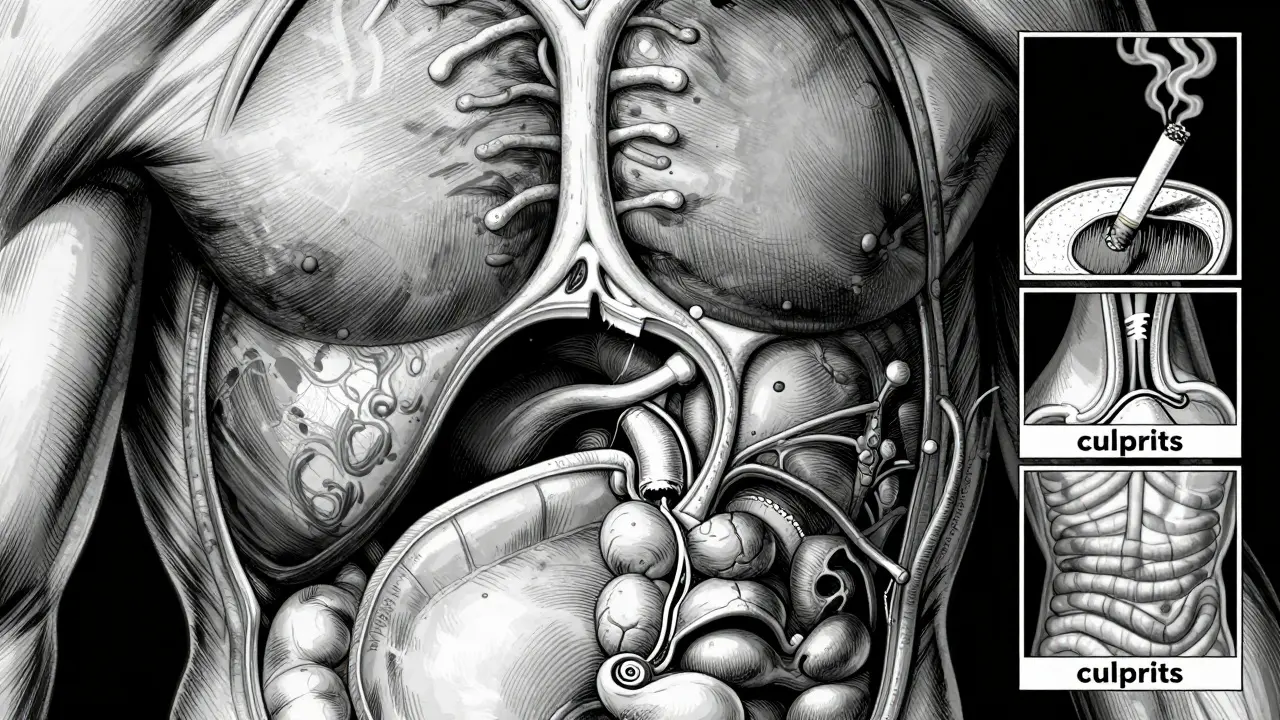
Several factors can weaken this valve. Obesity is a major culprit; having a BMI of 30 or higher can increase your risk by 2.5 times because of the extra pressure on the abdomen. Similarly, a Hiatal Hernia-where the top of the stomach pushes through the diaphragm-is present in nearly 94% of patients with erosive esophagitis. Even smoking doubles your risk by relaxing the LES and reducing saliva, which normally helps neutralize acid.
The Spectrum of Medication: From Quick Fixes to Powerhouses
Not all acid-reducing drugs work the same way. Depending on whether you have an occasional slip-up or a chronic condition, you'll likely encounter three main types of medication.
First, there are antacids like Tums. These are great for immediate relief because they neutralize the acid already sitting in your esophagus. However, they are short-lived and don't heal any underlying damage. Next are H2 blockers, such as Famotidine. These block histamine receptors to reduce the amount of acid your stomach produces, typically lasting 8 to 12 hours.
Then we have the heavy hitters: Proton Pump Inhibitors (PPIs). Drugs like Omeprazole and Esomeprazole don't just neutralize acid; they shut down the "pumps" (parietal cells) that create it. This allows the esophageal lining to heal. While H2 blockers might only reduce secretion by 60-70%, PPIs can knock it down by up to 98%.
| Medication Type | Example | How it Works | Duration of Effect | Healing Potential |
|---|---|---|---|---|
| Antacids | Tums, Rolaids | Neutralizes existing acid | Very Short (Minutes/Hours) | None |
| H2 Blockers | Famotidine (Pepcid) | Blocks histamine receptors | Medium (8-12 Hours) | Low to Moderate |
| PPIs | Omeprazole (Prilosec) | Inhibits acid-producing pumps | Long (24+ Hours) | High |
The PPI Paradox: Effectiveness vs. Long-Term Risks
PPIs are incredibly effective, but they aren't a "set it and forget it" solution. Many people stay on them for years, but medical experts warn against this. Long-term use (beyond one year) has been linked to a 20-50% increased risk of enteric infections and vitamin B12 deficiency. In older adults, high doses used for over three years are associated with a 35% increase in hip fracture risk.
One of the biggest traps is "rebound acid hypersecretion." If you've been on a PPI for months and stop cold turkey, your stomach may react by producing a massive surge of acid, making your symptoms feel worse than before you started. This is why doctors recommend a gradual taper over 4 to 8 weeks, often using an H2 blocker as a bridge to soften the landing.
Lifestyle Management: The Foundation of Recovery
Medication masks the symptoms, but lifestyle changes address the root cause. If you can manage your triggers, you might be able to reduce your reliance on drugs. Here is where the most significant impact happens:
- Weight Management: Losing just 5-10% of your body weight can reduce symptoms by half. It's the most effective non-drug intervention available.
- The Three-Hour Rule: Avoid eating within 2-3 hours of bedtime. This reduces nocturnal acid exposure by 40-60% because gravity helps keep food down while you digest.
- Trigger Identification: Common offenders include coffee, tomatoes, alcohol, chocolate, and spicy foods. While these affect 70-80% of patients, triggers are personal. Using a food diary for two weeks can help you spot your specific patterns.
- Sleep Elevation: If you wake up with a sour taste in your mouth, try elevating the head of your bed by 6 inches. Using a wedge pillow is more effective than just stacking extra pillows, which can actually kink your body and increase pressure on the stomach.
When Lifestyle and Pills Aren't Enough
For some, the LES is too damaged for meds to do the heavy lifting. When medication fails or when complications arise, surgery becomes an option. A Fundoplication is a common procedure where the top of the stomach is wrapped around the esophagus to create a new, stronger valve. It has a 90% success rate over 10 years. Newer options like the LINX device, a small ring of magnetic beads, provide a less invasive way to keep the valve closed.
You should be particularly vigilant if you develop Barrett's Esophagus. This is a condition where the lining of the esophagus changes to resemble the lining of the intestine to protect itself from acid. It's a precancerous state that occurs in 10-15% of long-term GERD cases and requires regular endoscopic monitoring.
Putting it All Together: A Step-by-Step Strategy
If you're struggling with reflux, don't just guess with over-the-counter pills. Follow a structured approach to get your life back.
- Track and Cut: Spend two weeks logging everything you eat and when your symptoms hit. Cut the most obvious triggers first.
- Optimize Your Routine: Stop eating at 7 PM if you go to bed at 10 PM. Walk for 15 minutes after meals to aid digestion.
- Strategic Medication: If using a PPI, take it 30-60 minutes before your first meal of the day. This is when the pumps are most active and the drug is most effective.
- Regular Review: Every 8 weeks, evaluate your progress with a healthcare provider. Ask if you can "step down" to a lower dose or an H2 blocker.
- Watch for Red Flags: If you experience difficulty swallowing (dysphagia), unexplained weight loss, or bleeding, seek an endoscopy immediately.
Can I take PPIs every day for the rest of my life?
Generally, no. While some people require long-term therapy for severe erosive disease, most should aim for the lowest effective dose for the shortest time. Long-term use is linked to B12 deficiency, bone fractures, and increased infection risk. Always discuss a "deprescribing" plan with your doctor.
Why does my reflux get worse when I stop my medication?
This is likely "rebound acid hypersecretion." Your stomach has spent months or years producing extra acid to compensate for the PPI. When the drug is removed, that extra capacity is unleashed. To avoid this, taper your dose slowly over several weeks.
Is drinking apple cider vinegar actually helpful for GERD?
There is limited clinical evidence to support this. For many, adding more acid (vinegar) to an already irritated esophagus can actually worsen the burning sensation. Stick to evidence-based lifestyle changes and medical therapies.
How do I know if I have GERD or just occasional acid reflux?
Occasional reflux happens to everyone. GERD is typically diagnosed when heartburn or regurgitation occurs at least twice a week. If symptoms persist despite over-the-counter treatments, it's time to see a specialist.
Can pregnancy cause acid reflux?
Yes, between 30-50% of pregnancies involve reflux. This happens due to both hormonal changes that relax the LES and the physical pressure the growing baby puts on the stomach.